A technique for fixation of the medial malleolar fracture is presented as an alternative to cannulated screws or conventional screw fixation. Two partially threaded screws are inserted in to the same corridors created by the temporary fixation after anatomic reduction. The procedure minimizes soft tissue stripping of the fracture fragments and facilitates expedient delivery of the hardware. In addition to the simplicity of the technique, there is substantial cost savings and better thread purchase compared to cannulated screws. (The Journal of Foot & Ankle Surgery 47(4):368–371, 2008)
Key Words: fracture fixation, medial malleolus
The he most common ankle fracture patterns are bimalleolar, bimalleolar equivalent (Supination external rotation [SER] with deltoid ligament rupture), or trimalleolar (SER-IV or pronation external rotation-IV) (1). These fracture patterns are often considered unstable and exhibit a transverse medial malleolar fracture that requires open reduction and internal fixation (ORIF) (1–3). The actual fixation technique, however, depends on both the fracture pattern and bone quality.
In healthy bone, stable fixation is obtained through two 4.0-mm partially threaded, cancellous screws placed perpendicular to the fracture line. The benefit to partially threaded screws is that overdrilling is not necessary, but compression is still obtained. If the fragment is not large enough to accommodate 2 screws, 1 screw and 1 Kirschner wire (K-wire) can be used. For those patients with poor bone quality, figure-of-eight tension band wiring can be employed instead to obtain stability and compression (3).
The standard method of ORIF for medial malleolar fractures can be broken down into 6 main steps.
- Excavation of fracture hematoma and removal of soft tissue interposition.
- Temporary fixation of an anatomically reduced fracture fragment with a K-wire or clamp.
- The 2.5-mm drill bit is used to create a pilot hole across the near and far fracture fragments.
- Screw length is determined with the depth gauge.
- A 4.0-mm tap is used to cut the thread pattern.
- Insertion of a 4.0-mm partially threaded cancellous screw.
- A second screw is then inserted in the same stepwise fashion if the size of the fracture fragment allows
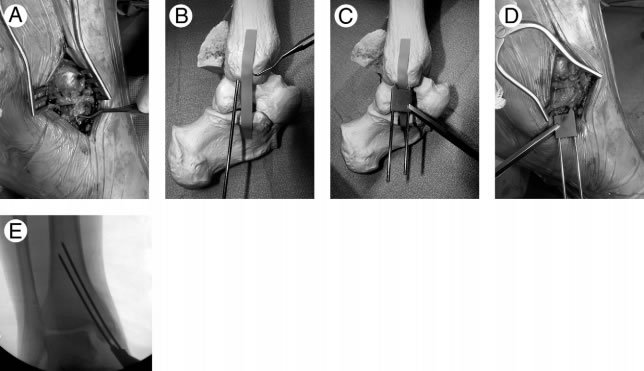
FIGURE 1 (A) Intraoperative photo of left ankle showing the manual pressure applied to the distal fracture fragment. (B) Bone model of left ankle with initial K-wire placement. The wire can be placed anteriorly or posteriorly. (C) Triple guide in place. (D) Intraoperative photo showing final placement of wires. (E) Fluoroscopic image demonstrating the level of insertion of the temporary fixation. In this instance both wires bowed as they contacted the lateral cortex of the tibia.
However, one of the difficulties of this approach is that there is often limited space for temporary fixation to remain in place while insertion of a second screw is performed. To obviate this “crowding” problem and make the process more efficient, a modified technique for temporary fixation placement has been used by the senior author (J.M.S.). This fixation technique for medial malleolar fractures facilitates permanent screw placement through the use of pilot holes created by temporary fixation. The steps are:
- The fracture is manually reduced and a bone pick is used to maintain proximal pressure on the distal fracture fragment (Figure 1, A). A 2.0-mm K-wire is placed across and perpendicular to the anatomically reduced fracture (Figure 1, B). The triple-guide is then placed over the wire in either the first or last hole in the guide, and a second 2.0-mm wire is then delivered through one of the remaining holes (Figure 1, C–D). The selection of the position of the K-wires in the triple drill guide should be based on the proposed final position of the screws. The wires are advanced until they penetrate or engage the far lateral cortex of the tibia (Figure 1, E). This will increase the stability of the temporary fixation and maintain reduction.
- The triple guide is removed, and the 3.5-mm drill sleeve is placed over one of the wires. The teeth of the drill sleeve are pressed against the malleolar fracture fragment (Figure 2).
- The wire within the drill sleeve is then removed and the 4.0-mm tap is placed directly into the drill sleeve and used to cut the thread pattern past the fracture line (Figure 3).
- After removal of the tap, the partially threaded screw, measuring 30 to 35 mm in length is placed into the hole.
Download PDF to continue reading report, footnotes, figures, tables, and references.
John M. Schuberth, DPM, has extensive experience in Complex Foot and Ankle Surgery. Throughout his 40 year career, he has performed over 25,000 surgical cases and over 1,500 ankle replacements. He has published extensively on a wide variety of subject involving foot and ankle surgery (128 publications) and lectured all over the world on Foot and Ankle surgery. Please refer to his most recent CV for details. Dr. Schuberth provides expert witness services to attorneys representing plaintiff and defense. His services include medical record review, thorough reporting, depositions, and trial testimony as needed. He has been deposed/testified over 20 times since 2020.
©Copyright - All Rights Reserved
DO NOT REPRODUCE WITHOUT WRITTEN PERMISSION BY AUTHOR.



